A common, treatable condition that can quietly signal much more about your overall health than you might expect.
Erectile dysfunction (ED) is one of the most common conditions affecting men, yet most men do not talk about it or raise it with their doctor, either because they are too embarrassed or because they wrongly believe it is simply a part of ageing about which nothing can be done. Managing ED is important in order to restore a man’s sex life, but equally it may point to a systemic health problem that needs to be addressed. This is why we can look at ED as a symptom of something wrong in the body rather than a disease in its own right; in other words, ED is a marker of your overall health.
What is ED?
ED is the persistent inability to achieve or maintain an erection sufficient for penetrative intercourse, causing distress to the man, his partner, or both. In other words, you either cannot get a hard erection at all, or you get one but lose it before completing intercourse — and this happens most of the time. Every man will occasionally encounter this through fatigue, stress or alcohol, but a one-off failure does not mean he has ED.
How common is the problem?
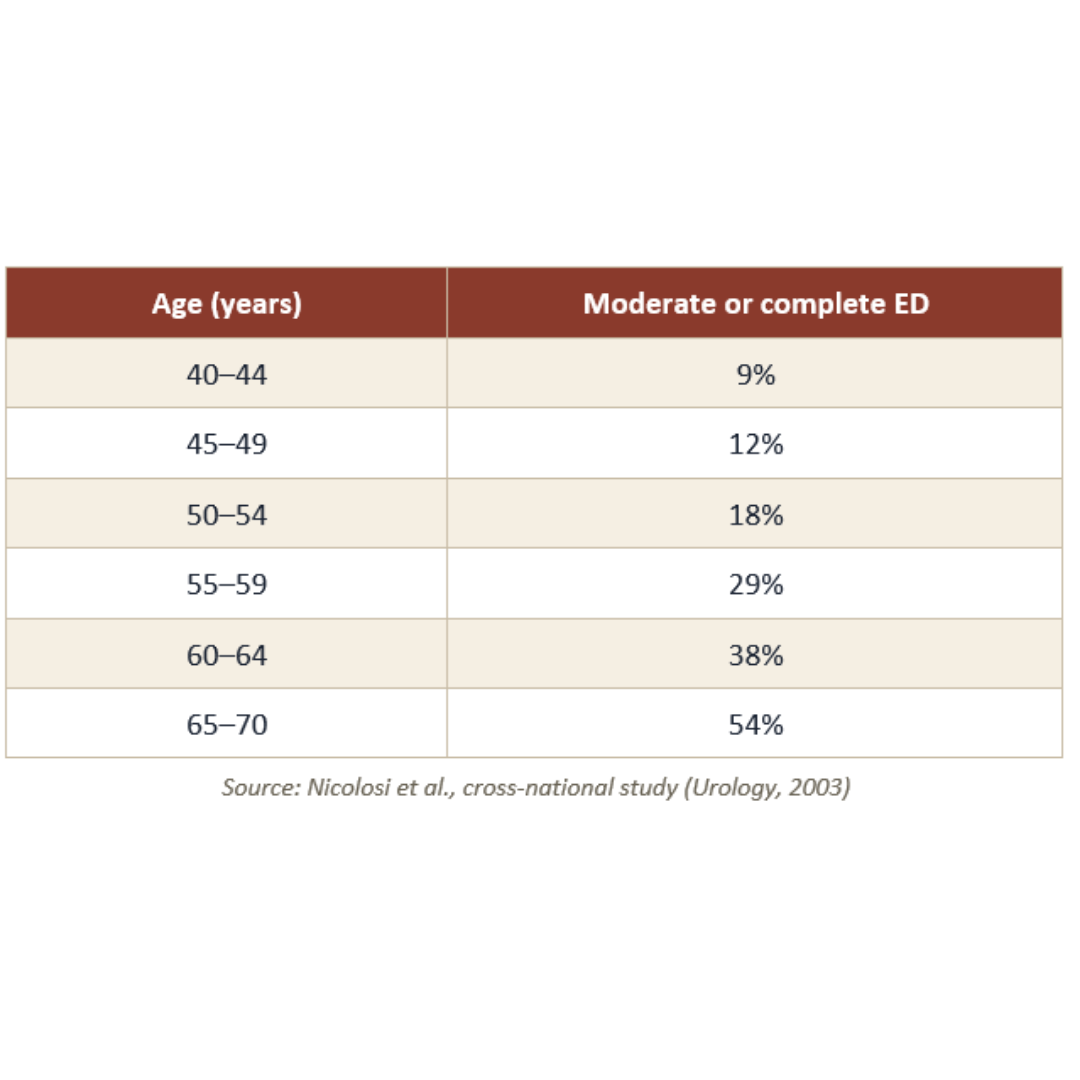
ED is one of the most common conditions in adult men, and its prevalence rises sharply with age. However, young men can also be affected, in what is known as primary ED, where the mechanism either does not work from the start or fails at a young age. The landmark Massachusetts Male Aging Study found that 52% of men aged 40–70 had some degree of erectile difficulty, with complete ED rising from 5% to 15% across that age range1. A subsequent study found that moderate or complete ED affected 9% of men aged 40–44, 18% by 50–54, 38% by 60–64, and 54% by 65–70 — an increase of roughly 10% per decade of life2. In the UK, a 2018 survey of 12,490 men reported that 41.5% had some degree of ED, with 7.5% reporting severe ED3, and globally the number of men affected was projected to reach 322 million by 2025, more than double the estimated 152 million in 1995.
What causes ED, and what are the risk factors?
An erection is a complex process that begins in the mind — hence the importance of a good psychological state. Signals then descend from the brain, along the spinal cord, and through the peripheral nerves that supply the penis, which is why an intact nervous system is essential. These nerves signal the blood vessels to dilate and pump blood into the penis, which is why an intact cardiovascular system is essential. Finally, normal penile anatomy is needed to trap and hold the blood, and this in part also depends on the male hormones. The sexual act itself requires good physical fitness. This is why, as I mentioned above, ED in most cases is a symptom of another disease rather than a disease in itself.
The causes therefore include cardiovascular, neurological, psychiatric and psychological, hormonal, respiratory, kidney and liver problems, as well as local penile problems such as Peyronie’s disease. Sometimes ED can occur as a side effect of a medication you are taking, such as anti-androgens, or of surgery, such as radical prostatectomy. In addition, lifestyle factors play a role, including smoking, alcohol, recreational drugs, poor diet, lack of exercise, chronic stress and poor sleep.
The psychological component in ED
In my professional opinion, the classification into “psychological” or “physical” is largely a textbook one; in real life the two components usually coexist and overlap, feeding each other and making the problem worse. That said, purely psychological ED is still seen, particularly in younger men with no underlying physical problem, where it usually arises from performance anxiety.
ED and infertility
ED is a cause of coital infertility, where conception fails because semen cannot be deposited in the vagina. However, it is important to note that the causes of ED also impair semen parameters and sperm health. For example, many of the causes of ED — such as diabetes, obesity and smoking — also impair sperm count, motility, morphology and DNA integrity. Diabetes can also impair ejaculation, causing anejaculation or retrograde ejaculation. Furthermore, the psychological pressure of trying to conceive, and of timing intercourse around ovulation, is itself a well-recognised cause of ED. In many cases I am called upon by IVF clinics to perform surgical sperm retrieval for men who cannot ejaculate, so that a sample can be obtained to fertilise their partner’s eggs.
Because both conditions often share the same risk factors, addressing the ED frequently improves sperm quality at the same time, since the same interventions help both.
Why ED matters beyond the bedroom
ED is most often a symptom of another health problem affecting your body, so it is not just about sex. Identifying and managing the risk factors is as important as treating the ED itself.
ED is now recognised as one of the earliest warning signs of cardiovascular disease. Studies suggest that ED often appears three to five years before a heart attack or stroke in men who go on to have one. This is because the arteries supplying the penis are only 1 to 2 millimetres wide, whereas the coronary arteries are 3 to 4 millimetres. When atherosclerosis develops throughout the body, the smaller penile arteries narrow first..
ED is also strongly associated with undiagnosed diabetes, hypertension, raised cholesterol, low testosterone, sleep apnoea and depression.
How is ED treated?
I always reassure my patients that all men with ED can be helped. But the most important step, before addressing the ED itself, is to diagnose any underlying risk factors and address them.
As for the management of ED itself, I like to follow a step-ladder approach, starting from the simplest options and progressing to the more invasive therapies. However, I also give my patients the option of choosing what they feel is best for them, so they do not necessarily have to follow my step-ladder approach; my role is to make them aware of the different options.
The step-ladder approach
Improving lifestyle and managing underlying health conditions - Weight loss, regular exercise, smoking cessation, moderating alcohol, and tighter control of diabetes, blood pressure and cholesterol, together with correcting low testosterone if present, can resolve mild ED on their own.
First-line treatment is the oral PDE5 inhibitors - sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra) and avanafil (Spedra).
Second-line options include vacuum erection devices, intracavernosal injections (Caverject, Viridal, Invicorp, Trimix), and intraurethral therapies (MUSE pellets or Vitaros cream).
Third-line treatment: when all of the above fail, penile prosthesis surgery is the way forward. It has satisfaction rates of over 90% and is a definitive solution.
Regenerative therapy: I have become a strong believer in penile rejuvenation therapy using low-intensity shockwave therapy (LiSWT) and platelet-rich plasma (the P-Shot), and I incorporate these into my treatment algorithms. It is important to be clear that the evidence for these treatments is still evolving — the data for shockwave therapy are very encouraging but not yet definitive, and platelet-rich plasma remains an emerging therapy. They will not work in every case, which is why patient selection and realistic expectations are very important.
Psychological support
As I have mentioned above, the psychological and physical components are intertwined, so in my practice I like to incorporate psychosexual counselling alongside medical and surgical treatments in many of my patients, in order to achieve the best possible outcome.
Written by Professor Amr Raheem
MB BCh, DipSurg, MSc, PhD
Fellow of the European Committee of Sexual Medicine (FECSM)
Fellow of the European Academy of Andrology (FEAA)
Fellow of the American College of Surgeons (FACS)
Consultant Andrologist
Professor in Andrology, Cairo University Hospital
References
1. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994;151(1):54–61.
2. Nicolosi A, Moreira ED Jr, Shirai M, Bin Mohd Tambi MI, Glasser DB. Epidemiology of erectile dysfunction in four countries: cross-national study of the prevalence and correlates of erectile dysfunction. Urology. 2003;61(1):201–206.
3. Mulhall JP, Goldstein I, Bushmakin AG, Yip CYY, Cordero J, Wong DG, et al. Prevalence, comorbidities, and risk factors of erectile dysfunction: results from a prospective real-world study in the United Kingdom. Adv Ther. 2022;39(6):2831–2849.
4. Ayta IA, McKinlay JB, Krane RJ. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999;84(1):50–56.
5. Montorsi P, Ravagnani PM, Galli S, Rotatori F, Briganti A, Salonia A, et al. The artery size hypothesis: a macrovascular link between erectile dysfunction and coronary artery disease. Am J Cardiol. 2005;96(12B):19M–23M.
6. Vlachopoulos CV, Terentes-Printzios DG, Ioakeimidis NK, Aznaouridis KA, Stefanadis CI. Prediction of cardiovascular events and all-cause mortality with erectile dysfunction: a systematic review and meta-analysis of cohort studies. Circ Cardiovasc Qual Outcomes. 2013;6(1):99–109.
7. Thompson IM, Tangen CM, Goodman PJ, Probstfield JL, Moinpour CM, Coltman CA. Erectile dysfunction and subsequent cardiovascular disease. JAMA. 2005;294(23):299Cardiol.
8. Zhao B, Hong Z, Wei Y, Yu D, Xu J, Zhang W. Erectile dysfunction predicts cardiovascular events as an independent risk factor: a systematic review and meta-analysis. J Sex Med. 2019;16(7):1005–1017.